

Introduction: The Most Searched A&P Questions
These are the anatomy and physiology questions that thousands of students, patients, and curious minds type into search engines every day. Here are clear, accurate, clinically relevant answers — written to be accessible to students at all levels, from introductory biology to advanced A&P.
1. What is the difference between anatomy and physiology?
Anatomy is the study of structure — what body parts exist, where they are, and how they relate to each other spatially. It answers the questions "what is it?" and "where is it?" Anatomy can be studied in a cadaver, where function is absent. Physiology is the study of function — how living structures work, the mechanisms by which they carry out their roles, and the processes by which they maintain homeostasis. It answers "how does it work?" and "why does it look the way it does?"
The two disciplines are inseparable because structure determines function. You cannot understand physiology without anatomy, and anatomy is meaningless without physiology. This is why the course is called Anatomy and Physiology.
2. What are the levels of organization in the human body?
From simplest to most complex:
- Chemical level: Atoms (H, C, O, N, Ca, P, etc.) and molecules (water, glucose, proteins, DNA, ATP)
- Cellular level: The cell — the smallest living unit. ~37 trillion cells in the human body
- Tissue level: Groups of similar cells performing a common function. Four tissue types: epithelial, connective, muscle, nervous
- Organ level: Two or more tissue types performing a specific function (e.g., heart, kidney, brain)
- Organ system level: Groups of organs cooperating for broader functions (e.g., cardiovascular system)
- Organism level: The complete, living individual
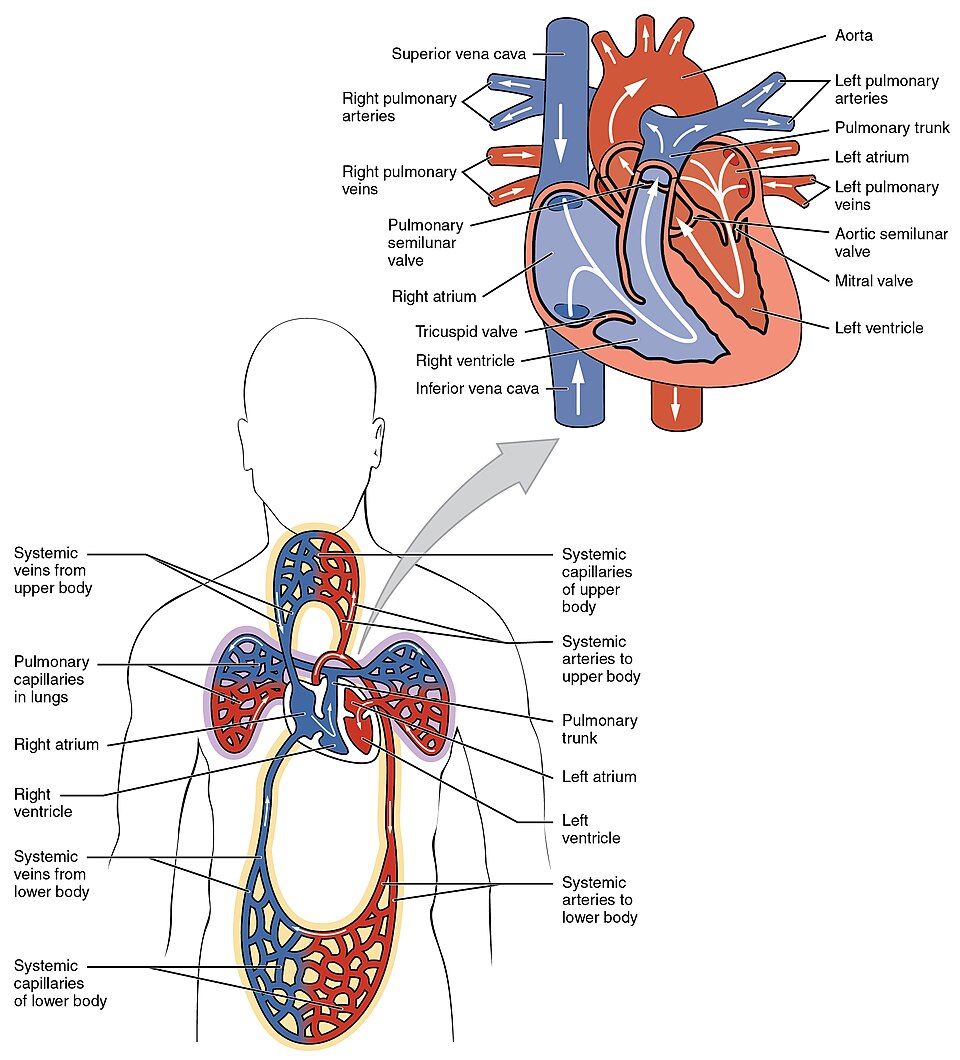
3. What is the difference between arteries and veins?
Arteries carry blood away from the heart. They carry oxygenated blood in the systemic circulation (the major exception: the pulmonary artery carries deoxygenated blood from the right ventricle to the lungs). Arteries have thick, elastic, muscular walls to withstand high pressure. The largest artery is the aorta (~2.5 cm diameter).
Veins carry blood toward the heart. They carry deoxygenated blood in the systemic circulation (the major exception: pulmonary veins carry oxygenated blood from the lungs to the left atrium). Veins have thinner, less muscular walls and contain one-way valves that prevent backflow against gravity. Veins carry ~64% of total blood volume at any given time (the blood reservoir).
Memory trick: A for Away (Arteries carry blood Away from the heart).
4. How do the kidneys filter blood?
Each kidney contains approximately 1 million nephrons — the functional units of filtration. Here is the sequence:
- Glomerular Filtration: Blood enters the glomerulus (a capillary tuft) at high pressure. Approximately 20% of plasma is pushed through the glomerular filtration membrane into Bowman's capsule (the funnel surrounding the glomerulus). This creates about 180 liters of filtrate per day. Large molecules (proteins, blood cells) cannot pass through and remain in the blood.
- Tubular Reabsorption: As filtrate moves through the proximal convoluted tubule, loop of Henle, and distal convoluted tubule, ~99% is reclaimed back into the peritubular capillaries. This includes all glucose (at normal blood levels), all amino acids, 99% of filtered water, and most ions. The proximal tubule handles most reabsorption (~65% of Na⁺ and water).
- Tubular Secretion: The tubule actively secretes additional waste products from peritubular capillaries into the tubular fluid — including H⁺ (acid-base regulation), K⁺, creatinine, and some drugs.
- Concentration: The collecting duct (under ADH influence) determines the final water reabsorption, concentrated the urine. The remaining ~1–2 liters/day is urine, containing urea, creatinine, excess ions, and other metabolic waste.
5. What causes muscle cramps?
A muscle cramp is an involuntary, sustained, painful muscle contraction. The most common causes:
- Electrolyte imbalances: Low sodium (hyponatremia), potassium (hypokalemia), calcium (hypocalcemia), or magnesium (hypomagnesemia) alter the membrane potential of muscle cells and motor neurons, increasing excitability and causing spontaneous contractions. This is why cramps are common during prolonged exercise with excessive sweating, or in people taking diuretics.
- Dehydration: Reduces extracellular fluid volume, concentrating electrolytes and reducing blood flow to muscles.
- Muscle fatigue: Fatigue impairs motor neuron control mechanisms, possibly allowing excessive alpha motor neuron firing. This is the likely mechanism for exercise-induced cramps in well-hydrated, electrolyte-replete athletes.
- Poor circulation: Nocturnal leg cramps are often related to reduced blood flow to the lower extremities.
Treatment: Stretching activates Golgi tendon organs, which inhibit alpha motor neurons via Ib afferent fibers — reflexively relaxing the cramping muscle. Hydration and electrolyte replacement address the underlying cause.
6. What is the difference between Type 1 and Type 2 diabetes?
Both types involve failure of blood glucose homeostasis, but through different mechanisms:
Type 1 Diabetes Mellitus: An autoimmune disease in which T cells destroy the insulin-producing beta cells of the pancreatic islets of Langerhans. Results in absolute insulin deficiency — zero insulin production. Blood glucose rises uncontrolled (hyperglycemia). Without insulin, cells cannot absorb glucose; the body catabolizes fat instead → ketone body production → diabetic ketoacidosis (DKA), which can be fatal. Typically diagnosed in childhood or adolescence (but can occur at any age). Requires exogenous insulin for life. Accounts for 5–10% of diabetes cases.
Type 2 Diabetes Mellitus: Begins with insulin resistance — cells (especially muscle, liver, and fat cells) become less responsive to insulin, requiring more insulin to achieve the same glucose-lowering effect. The pancreas compensates by producing more insulin. Over years, the beta cells become exhausted and fail to keep up → relative insulin deficiency → hyperglycemia. Strongly associated with obesity (particularly visceral adiposity), physical inactivity, and genetics. Initially manageable with lifestyle modification and oral medications (metformin, SGLT2 inhibitors, GLP-1 agonists). Accounts for 90–95% of diabetes cases. Progressive — many eventually require insulin.
7. How does the immune system fight a virus?
The immune response to a viral infection unfolds in overlapping waves:
Innate Immune Response (Hours to Days):
- Pattern recognition receptors (especially Toll-like receptors) on macrophages and dendritic cells detect viral nucleic acids (dsRNA, ssRNA) — molecular patterns not present in human cells.
- Detection triggers secretion of interferons (type I: IFN-α and IFN-β) — signaling proteins that warn neighboring cells to upregulate antiviral defenses.
- Natural killer (NK) cells patrol for and destroy cells that have downregulated MHC-I expression (a common viral evasion tactic) — NK cells kill without prior sensitization.
- Inflammation brings neutrophils and macrophages to the infection site.
Adaptive Immune Response (Days to Weeks):
- Dendritic cells engulf virus-infected cells, process viral proteins, and present peptide fragments on MHC molecules. They migrate to lymph nodes and activate naive T cells.
- CD4⁺ Helper T cells (activated by MHC II + viral peptide) coordinate the response — they activate B cells and cytotoxic T cells and secrete cytokines that amplify the response.
- CD8⁺ Cytotoxic T cells (activated by MHC I + viral peptide) identify and destroy virus-infected cells throughout the body before the virus can replicate further.
- B cells (activated by T helper cells and direct antigen binding) differentiate into plasma cells that secrete antibodies — immunoglobulins that bind specifically to viral surface proteins, neutralizing the virus and marking it for destruction by phagocytes (opsonization).
- After the infection is cleared, long-lived memory B and T cells persist in the body for decades, enabling a faster and more powerful response if the same virus is encountered again. This immunological memory is the basis of vaccination.
8. What does the liver do?
The liver is the body's master metabolic organ — it performs over 500 distinct functions. Key functions include:
- Detoxification: Processes and neutralizes drugs, alcohol, environmental toxins, and metabolic waste products. Phase I enzymes (cytochrome P450s) chemically modify toxins; Phase II enzymes conjugate them to water-soluble molecules for excretion.
- Protein synthesis: Produces ~90% of all plasma proteins, including albumin (maintaining oncotic pressure), clotting factors (fibrinogen, prothrombin), transport proteins, complement proteins, and C-reactive protein.
- Glucose regulation: Stores glucose as glycogen (glycogenesis) after meals; releases glucose from glycogen during fasting (glycogenolysis); synthesizes new glucose from amino acids and glycerol (gluconeogenesis). The liver is the primary blood glucose buffer.
- Lipid metabolism: Synthesizes VLDL (very low-density lipoproteins) that transport triglycerides; processes chylomicron remnants from dietary fat absorption; produces cholesterol; synthesizes bile acids from cholesterol.
- Bile production: Produces ~500–1000 mL of bile per day, which is stored in the gallbladder and released into the duodenum to emulsify dietary fats, enabling lipase activity and fat-soluble vitamin absorption.
- Vitamin storage: Stores significant quantities of fat-soluble vitamins (A, D, E, K) and vitamin B12.
- Immune function: Contains Kupffer cells (resident macrophages) that clear bacteria, endotoxins, and cellular debris from the portal blood.
9. Why do we feel pain?
Pain is not a tissue event — it is a brain event. The sensation of pain requires the activation of nociceptors (free nerve endings that detect potentially harmful stimuli) and transmission of signals through the spinal cord to the brain, where the signal is interpreted as pain. Three types of stimuli activate nociceptors:
- Mechanical: Pressure, cutting, crushing
- Thermal: Extreme heat or cold (above ~45°C or below ~10°C)
- Chemical: Inflammatory mediators — prostaglandins, bradykinin, histamine, substance P — sensitize nociceptors after tissue injury, creating inflammatory pain (allodynia and hyperalgesia).
Pain signals are transmitted via two fiber types: A-delta fibers (myelinated, fast — the sharp, immediate pain of a finger prick) and C fibers (unmyelinated, slow — the dull, throbbing pain that follows). The gate control theory (Melzack and Wall, 1965) explains why rubbing an injured area reduces pain: large-diameter mechanoreceptor fibers (A-beta) activated by rubbing inhibit pain transmission in the dorsal horn of the spinal cord.
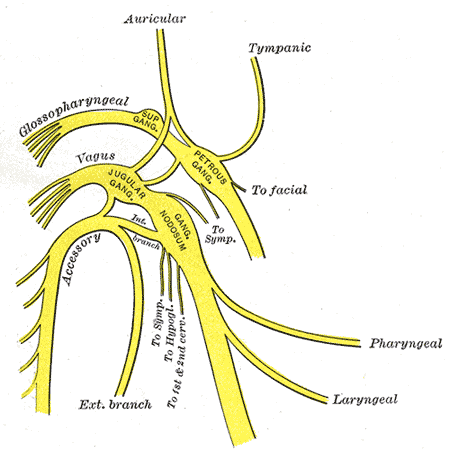
10. What is the autonomic nervous system?
The autonomic nervous system (ANS) controls involuntary functions — the processes that run continuously without conscious effort or awareness. It has two main divisions:
Sympathetic Division ("Fight or Flight"): Activated by stress or physical exertion. Effects: increased heart rate and force; bronchodilation; pupil dilation; inhibited digestion; increased blood glucose; increased sweat; piloerection. Cell bodies in the thoracolumbar spinal cord (T1–L2). Preganglionic fibers are short; postganglionic fibers are long. Main neurotransmitters: ACh (preganglionic) → norepinephrine (postganglionic) + epinephrine from adrenal medulla.
Parasympathetic Division ("Rest and Digest"): Active during rest and recovery. Effects: decreased heart rate; bronchoconstriction; pupil constriction; stimulated digestion; increased glandular secretions; promotes voiding (urination, defecation, sexual arousal). Cell bodies in the brainstem (cranial nerves III, VII, IX, X) and sacral spinal cord (S2–S4). Long preganglionic fibers; short postganglionic fibers. Neurotransmitter: ACh at both synapses.
Most organs receive dual innervation from both systems — they generally produce opposing effects and the balance between them determines organ activity. The vagus nerve (CN X) carries approximately 75% of all parasympathetic fibers.
Discussion (0)
Leave a Comment